Source: The Star Online
A clinical study shows that it is possible to regenerate cartilage in damaged joints using patients’ own blood stem cells.
WE might never be able to regrow lost limbs the way lizards regrow their tails, but the fact that certain parts of our body can heal from injuries is not science fiction.
Some of these processes kick in whenever there is an injury. If we cut ourselves, new skin cells can be generated to replace lost ones. If we donate part of our liver, the cells in the remaining part have the ability to multiply and regenerate the whole organ.
However, some will only heal when the injury isvery severe. This is the case with articular (joint) cartilage, the biological cushion that covers the surface of our bones where they meet in joints, like the ones in our hips and knees.
“The progressive thinning of the articular cartilage (in the case of osteoarthritis) initially does not cause pain, until the arthritis has progressed to an extent where the underlying bone (with nerve fibres) is exposed,” said Dr Saw Khay Yong, an orthopaedic surgeon from Kuala Lumpur. “In trauma, severe injury will normally cause bone bruising (which will cause pain) in addition to articular cartilage damage.”
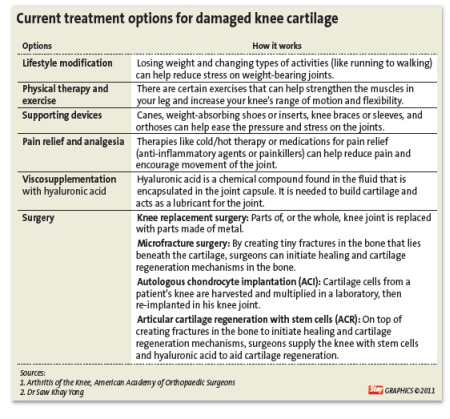
 In this photo published in the Arthroscopy: Journal of Arthrosopic and Related Surgery, surgeons drilled holes in the bone of a knee joint (left) to initiate cartilage repair. After that, stem cells and hyaluronic acid are injected into the operated knee. Two years after the operation, Dr Saw and his colleagues are able to show cartilage repair as white cartilage is once again seen covering the underlying bone (right ). – Photo with permission from the authors
In this photo published in the Arthroscopy: Journal of Arthrosopic and Related Surgery, surgeons drilled holes in the bone of a knee joint (left) to initiate cartilage repair. After that, stem cells and hyaluronic acid are injected into the operated knee. Two years after the operation, Dr Saw and his colleagues are able to show cartilage repair as white cartilage is once again seen covering the underlying bone (right ). – Photo with permission from the authorsUnfortunately, the stem cells located in the bone marrow in the knee are not capable of initiating sufficient repair to replace the lost cartilage. “This is the reason why patients are left with prolonged cartilage loss that leads to a painful or swollen joint,” he explained.
Since two decades ago, orthopaedic surgeons have been using this knowledge to their advantage. Besides asking their patients to decrease activity and lose weight, or injecting their patients’ knee with “lubricant” fluids like hyaluronic acid and anti-inflammatory substances like cortisone, they drill through remaining cartilage to reach the bone to initiate the healing and cartilage regeneration mechanism with a technique called microfracture.
The limitation to this technique is that there is a chance the patient’s bone marrow may replace the lost cartilage (hyaline cartilage) with a weaker, less flexible type of cartilage called fibrocartilage, said Dr Jeb Broyles, a US orthopaedic specialist from Louisiana.
Dr Broyles was attracted to Malaysia by the results of a Malaysian clinical study on a technique that appears to improve on existing procedures.
The study was led by Dr Saw, who has shown, together with researchers from Universiti Putra Malaysia (UPM), that they could regenerate normal cartilage in patients’ knees by injecting the patient’s own blood stem cells into their knees after drilling holes into the underlying bone.
Dr Broyles was here to learn the technique.
From goats to humans
Before trying the procedure (called Articular Cartilage Regeneration with Autologous Peripheral Blood Progenitor Cells and Hyaluronic Acid after Arthroscopic Subchondral Drilling, or ACR in short) in humans, Dr Saw and researchers from UPM tried to regenerate cartilage in the knee joints of goats in 2005.
They harvested stem cells (bone marrow progenitor cells or BPMC) from goat bone marrow and injected them into the goats’ knees, together with hyaluronic acid (a compound needed to build cartilage), after drilling holes in the cartilage and bones of their knee joints.
After observing and documenting evidence of good cartilage repair in goats, Dr Saw and his team then proceeded to perform a pilot study on 10 patients. However, instead of using BMPC, Dr Saw tried using stem cells harvested from his patients’ own blood (peripheral blood progenitor cells or PBPC), as it is safer and easier to harvest.
“Recent study into the properties of these PBPCs has shown that they are similar to embryonal stem cells in that they express transcription factors specific to pluripotential cells, have proliferative potential, have the ability to differentiate into a multitude of cell types, and are more immature than BPMCs,” wrote Dr Saw and his team in a paper on the pilot study, published in the Arthroscopy Journal of Arthrosopic and Related Surgery early this month.
The paper published the biopsy results of five of the patients who participated in the pilot study. “All of our biopsy specimens showed histologic features of hyaline cartilage …” the researchers wrote.
 For those with very bad knees, knee replacement surgery may be the only option.
For those with very bad knees, knee replacement surgery may be the only option.One of the first patients who participated in the pilot study is 38-year-old Joanna Hart, an expatriate who was told she needed a knee replacement four years ago.
The cartilage that prevented the bones in her left knee from rubbing against each other had worn off due to a less than satisfactory surgery she had to set her recurrently dislocated kneecap in place. As a result, she couldn’t fully straighten her legs.
As she was not keen on having her knees replaced, Hart decided to try the new procedure – then in its final stages of research in goats. “My knee has gradually improved over the last four years, and I had a second surgery two years ago to complete the stem cell therapy,” she told Fit4Life in a recent email. (Both surgeries targeted different areas of her knee joints.)
Two years after her first surgery, she was able to climb up the stairs to Batu Caves. Now, back in Scotland, she does five to eight gym classes a week, goes horse riding, and does a lot of walking. “I can run without pain now too, but I don’t do very much of that,” she added.
“A majority of patients show progressive improvements, even up to three to four years, as opposed to the microfracture technique. International Knee Documentation Committee (IKDC) results ( scores used to chart patients’ progress and long term results) following microfracture tend to deteriorate after two years,” said Dr Saw.
Nevertheless, in his experience, two patients had had bad falls onto their operated knees one year after surgery, and their knee function deteriorated. “Another middle-aged patient with a previous infected knee, who had underwent multiple surgeries, had a recurrence of bone spur and the patient chose to have a total knee replacement,” he noted.
Inducing repair, slowly
The steps involved in ACR may be simple, but the process of recovery is one that is long and time consuming.
“It normally takes one or two years before patients can return to their normal sporting activities,” explained Dr Saw.
Before suggesting the procedure, orthopaedic surgeons have to assess their patients to determine if they need surgery to rectify their problem. “There are patients who only need physiotherapy or hyaluronic acid injections,” he noted.
Other treatment options include going on therapy or medication to help reduce the pain and discomfort, using supportive devices such as knee braces and orthoses to ease the stress or pressure on the joint.
However, for those whose injuries are severe enough to warrant cartilage regeneration or replacement surgery, they have the options of going for a knee replacement surgery or cell-based regeneration therapies like the ACR and autologous chondrocyte implantation (ACI).
In an ACI procedure, a patient’s cartilage cells is harvested from the knee joint, multiplied in a lab, and re-implanted into the affected knee.
“If their knees are bad enough to require a total knee replacement, there is no point in doing ACR. But there are a lot of patients who do not need a total knee replacement, and this is especially so for people who are in their 30’s or 40’s,” said Dr Saw.
First, a patient will have to undergo a minimally invasive “keyhole” surgery to enable the surgeon to drill holes into the bones in their knees. One week after the surgery, the stem cells (PBPCs) in his blood will be harvested and injected (together with hyaluronic acid) into his knee.
For the following four to five weeks, the patient will be given physiotherapy for two hours daily, and weekly stem cell and hyaluronic acid injections. (see How do doctors regenerate your cartilage with stem cells)
“The risks are generally the same as any other minimally invasive procedures,” said Dr Saw.
Still, according to a patient information sheet distributed to participants of an ongoing randomised controlled trial, problems do occasionally occur, and there is a risk of infections, unsuccessful surgery, or less than satisfactory recovery.
Although minor complications (like transient pain after surgery, the “locking” of the knee joint, and swelling that resolves within three to six months of surgery) are common, major complications like recurrent effusions (accumulation of fluid in the joint), infections, and blood clots are rare.
Nevertheless, if the surgery is unsatisfactory, it is usually still possible for patients to undergo other types of cartilage repair surgery.
Even so, Dr Saw said that there were no cases of infections or significant adverse events in the 50 patients recruited for the trial.
Looking forward, working backwards
While Dr Saw and his co-authors acknowledged in their latest paper that the sample size (five patients) was too small and there were no control group to compare their results, Dr Saw is convinced that it works.
But even though he thinks that ACR has great potential, he also acknowledged that it is only one of the several treatment approaches for managing cartilage injuries in joints – another tool in the bag.
“Right now, based on our studies, we know that it works,” he said. But Dr Saw and his team want to know why and how ACR works, and how it compares to existing procedures. So, the next step for them is to understand the science behind the procedure by doing animal studies.
“We are in the midst of completing a randomised clinical trial and writing a book chapter on cartilage regeneration,” Dr Saw revealed.
On top of that, he is also working with other doctors and equipment suppliers to design specific instruments for the procedure, as they are still using modified instruments.
“Now, we are basically in the process of improving the technique,” he said.
Even with international interest – surgeons from the US and countries in the region have visited Malaysia to learn about the procedure – ACR has yet to be performed in other countries due to regulatory requirements.
“We are collaborating with Prof Gary Poehling at Wake Forrest University and Dr David McGuire from Anchorage, Alaska, in the set up of a multi-centre trial,” said Dr Saw.
Currently, we are collecting safety data from our patients in Kuala Lumpur for Wake Forrest University to present to the US FDA, he explained.